Starting January 2026, CMS allows radiologists to supervise contrast imaging procedures remotely using video technology—but only if specific on-site personnel are present. Imaging centers say they’re ready, but technologists remain concerned about one issue.
The framework for contrast supervision in radiology is changing. With recent regulatory updates from CMS and new guidelines from the American College of Radiology (ACR), practices are working towards implementing virtual supervision models. Understanding the rules, their effects, and modalities is essential to maintaining safety while expanding patient access.
The Centers for Medicare & Medicaid Services (CMS) has permanently adopted a definition of direct supervision that permits real-time, two-way audio-visual telecommunications for many services, effective January 1, 2026. This decision applies to diagnostic tests, incident-to services, and pulmonary/cardiac rehabilitation, though it generally excludes services with 10- or 90-day global surgery indicators.
This policy provides practices with long-term planning certainty, moving beyond the temporary pandemic-era flexibilities. The CMS ruling specifically requires real-time audio and visual interactive telecommunications, excluding audio-only communication, to ensure supervising physicians can adequately assess patients and respond to adverse events.
The ACR maintains that direct supervision is required whenever contrast material is administered. Their 2025 guidance supports virtual direct supervision, provided a physician performs it and involves only one level of virtuality—meaning an off-site physician should not be supervising an off-site licensed practitioner.
Traditional direct supervision requires the physician to be present in the office suite and immediately available. Virtual supervision meets this "immediate availability" standard through technology, allowing for continuous oversight during contrast administration.
While CMS provides flexibility on the location of the supervising physician, professional standards from the ACR and ASRT emphasize the need for qualified on-site personnel beyond the radiology technologist. Many institutional policies now require at least one on-site licensed practitioner (such as an NP, PA, or CNS) with formal training in patient assessment and emergency response.
These practitioners must be able to recognize and manage adverse reactions to contrast material. This includes the ability to administer emergency medications—such as antihistamines, IV fluids, and epinephrine—under standing orders or institutional protocols.
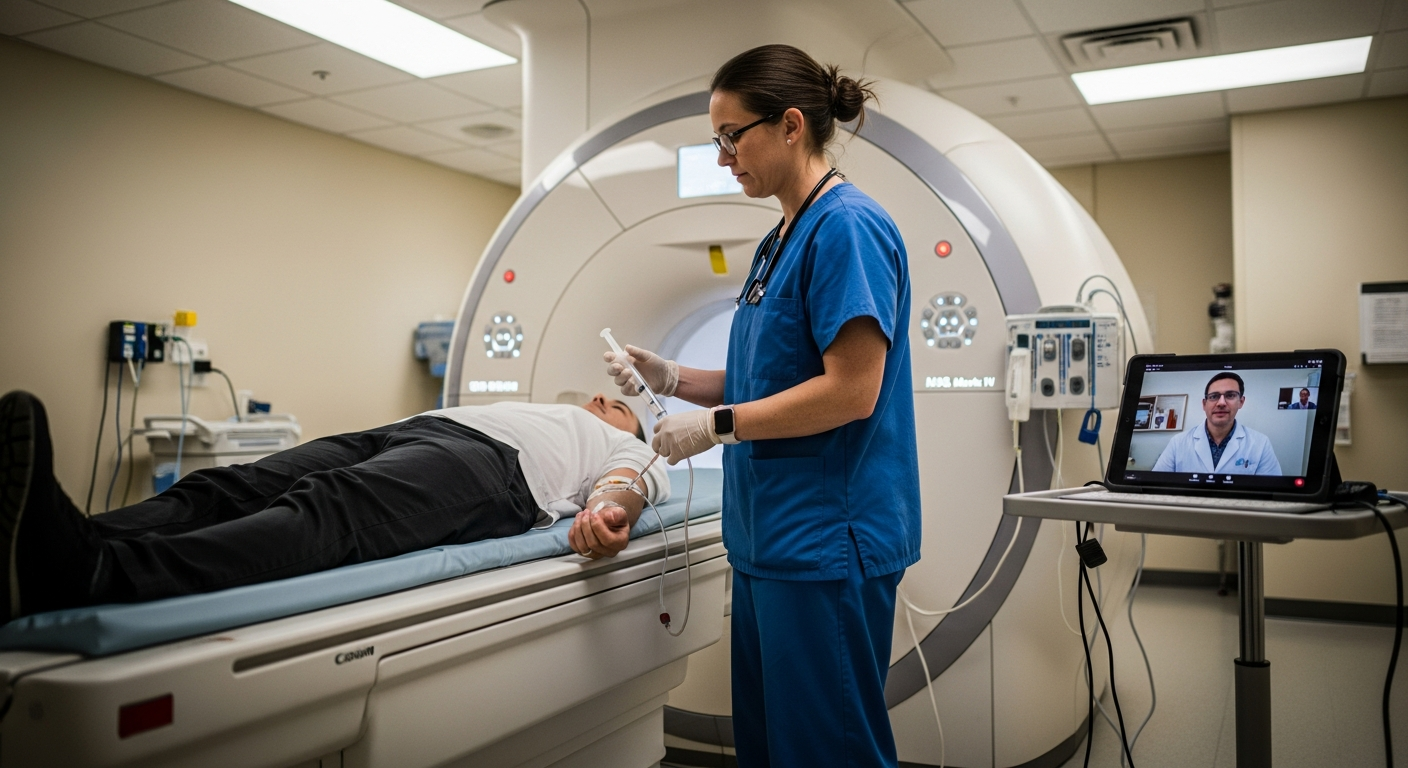
The primary modality for virtual direct supervision is real-time, two-way audio and visual interactive telecommunications. This technology must enable the supervising physician to communicate directly with the on-site personnel responsible for patient safety. Successful implementation requires reliable video equipment, high-speed internet, secure PACS access, and HIPAA-compliant communication platforms.
Virtual supervision addresses radiologist shortages, particularly in rural communities, by enabling remote oversight. This geographic flexibility allows specialized radiologists to provide expertise across multiple locations, helping to ensure that patients in remote areas receive timely access to contrast-enhanced imaging.
Virtual supervision can improve workflows by allowing more flexible scheduling and extended operating hours. Radiologists can provide oversight for multiple facilities, optimizing their time while maintaining safety standards. These efficiency gains can reduce scheduling conflicts and improve patient throughput, even when facilities face staffing challenges.
While radiologists may have mixed feelings about remote contrast supervision, technologists often express more significant concerns about virtual supervision models. The American Society of Radiologic Technologists (ASRT) has raised specific concerns about ensuring qualified healthcare personnel are available for immediate treatment of adverse events and does not support remote supervision of radiologic technologists unless other qualified personnel are physically present.
These concerns underscore the importance of strong working relationships, training, and ongoing reassurance for technologists adapting to virtual supervision environments. Success requires addressing these concerns through clear communication protocols, robust support systems, and emergency response procedures that maintain technologist confidence.
Effective emergency response in virtual environments requires detailed planning and clear escalation procedures. The supervising physician must be able to direct care through the qualified on-site personnel. Regular training and simulation exercises help ensure that all staff understand their roles and can execute emergency procedures effectively, even when the physician is not physically present.
Successful virtual supervision implementations require robust training programs for on-site technologists covering contrast reactions, clear communication with remote physicians, and established emergency escalation procedures. Infrastructure investments in high-quality audio-visual equipment, reliable internet connectivity, and secure communication platforms form the foundation of effective virtual supervision programs.
Best practices include regular competency assessments, ongoing education programs, and continuous quality improvement initiatives that ensure virtual supervision maintains the same safety and efficacy standards as traditional on-site supervision. These approaches help build confidence among staff while ensuring optimal patient outcomes.
The shift toward virtual contrast supervision offers radiology practices greater operational flexibility while maintaining rigorous safety standards. As practices adapt to these new regulatory frameworks, the focus must remain on patient safety, staff confidence, and clinical excellence. When appropriately executed, virtual supervision is the future of cost-effective and patient-focused imaging services across the country. Whether hospitals and imaging centers adapt quickly enough is the question that awaits an affirmative answer.